Print
Print Email
EmailI have previously written on the enormous uncertainty surrounding the COVID-19 pandemic in Africa. Here I speak directly to data and knowledge gaps that need to be filled and can be filled through concerted joint action among researchers, African governments and public agencies, and bilateral and multilateral development partners. The emphasis here is on using data to generate better decision tools, meaning that data collection needs to be informed and driven by the needs of these model(ing)- based decision tools.
The baseline assumption that drives these comments is that COVID-19 will be present and rapidly changing in Africa for well over a year and perhaps longer, meaning that there is both time and need to fill data and knowledge gaps to better inform responses in real time, including responses related to food supply chains (FSCs). Broad consensus exists across informed observers and scientists on this point. The key contention underpinning the piece is that one cannot understand or anticipate the impact of COVID-19 on African FSCs without understanding and anticipating its impact on three areas: (1) morbidity and mortality, (2) human behavioral responses to the disease and to government actions around it, and (3) the spending power and livelihoods of most citizens. The conclusion is that we therefore need more data, and more modeling with that data, to make informed judgements about what steps to take in the short- and medium runs. (An aside is that the enormous structural investment needs of African FSCs mean that many long-run needs and recommendations are not particularly sensitive to the details of the COVID-19 pandemic).
Here I emphasize three types of data and modeling that are needed. The first relates to the virus and disease themselves: drivers of transmission, morbidity and mortality. On the question of transmission, we must realize that food markets need to remain open even as they serve as potentially huge, ongoing “amplification events” that can spur exponential growth in infection. This is especially the case in the large, crowded, urban informal markets where most low-income consumers make their purchases. The impact of these markets on transmission can be modeled but requires data on flows over time, and resulting densities, of people in different shopping areas. “Good enough” data on this can be collected in safe and relatively cheap fashion through population-based cellphone surveys (see my colleague Mywish Maredia’s blog post on this) and also through spatially targeted, regular mapping / counting exercises. These need to be designed based on knowledge of the existing food trading system, coordinated with policy makers, carried-out regularly, and linked to rapid and largely automated processing both to feed into modeling and to inform policy makers.
Regarding morbidity and mortality, it is a shocking fact that we still have no systematic modeling of the impact of Africa’s many co-morbidities on the Covid-19 fatality rate. The only models that have adapted to African conditions (e.g. Walker et. al. from late March) incorporate the continent’s younger age structure, which dramatically reduces estimated death rates. No modeling effort that I have seen addresses the impact of co-morbidities – HIV/AIDS, tuberculosis, malaria, under-nutrition, rising overweight and obesity and related diabetes and hypertension, among others. We know that these will increase mortality, we have initial estimates for at least some of them from developed economies, but I have not seen anyone bring this information together into an informed “best guess” about their net impact on the effects of COVID-19. The result is that we do not know if COVID-19 will be more or less deadly in Africa compared to more developed economies. This is a major, and resolvable, knowledge gap. (I note that PreventEpidemics, in collaboration with Africa CDC, WHO, and others, has launched Partnership for Evidence-Based Response to COVID-19 (PERC) in Africa. This may be a logical place to house this effort and incorporate this kind of modeling into design of response options).
The second major data and knowledge gap regards human behavior: how are people responding to their knowledge and fears about the disease, and to government policies and actions? Here, Google’s weekly “Community mobility reports” data is now available for over 130 countries, for free download. These data provide fairly dramatic evidence for the impact of more- vs. less severe PHSMs (public health and safety measures) on the movement of citizens, as shown below: Rwanda, South Africa, Uganda, Zimbabwe, and Botswana all show dramatic, rapid reductions in citizen mobility following announcement of lockdowns, while Zambia and Tanzania, which have taken much less aggressive stances, show much smaller declines in mobility.
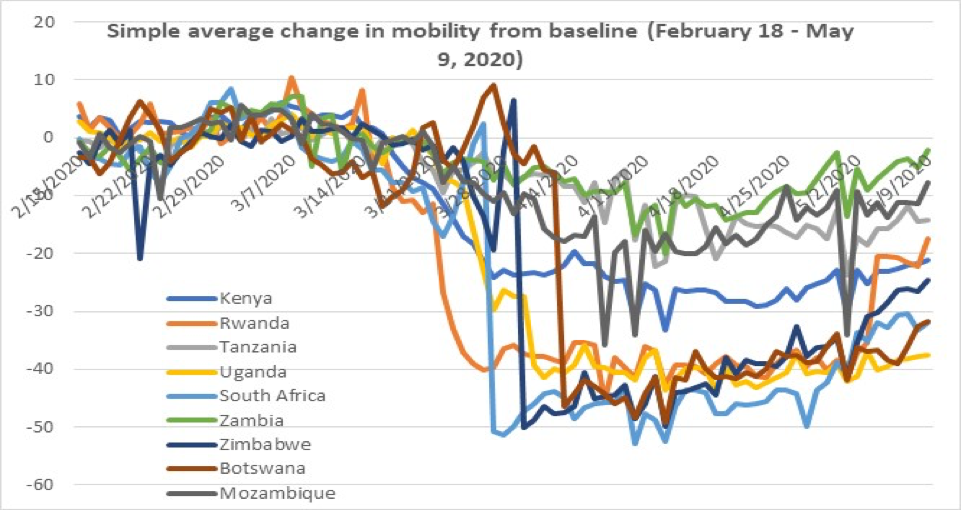
So these data are tremendously useful. However, they are also biased and not spatially specific in the great majority of African countries. They are biased because they are based on users of smartphones, who have higher income, are more educated, and more urban than owners of feature phones or those who do not own any cellphone. We thus have essentially no data on the mobility of the great mass of lower income consumers that do not have smartphones and likely have less ability – due to sheer economic necessity to continue working - to limit their movement. A key point here is that regular population-based cellphone surveys can be an effective way to rapidly generate data among this demographic, as they are not limited to smartphone users. But if they are to be useful, these efforts need to be organized through collaborative efforts that include research organizations and governments and their responsible agencies.
The Google mobility data lack spatial specificity in that most African countries feature single weekly values for the entire country. Nigeria and Kenya are important exceptions to this pattern, each having data for the country as a whole and many administrative subdivisions. This is important because we have to expect that responses may vary quite a lot between different size cities, across regions, and between rural and urban areas.
The point is that informal food markets, with their necessary congregations of large numbers of people, are ongoing amplifying events for the spread of the virus. We thus need data on flow in and out and resulting density of people in identified market locales. As noted above, these data can be connected in timely and affordable fashion through cellphone surveys combined with simple, targeted counting / market mapping exercises.
The third area of need for data and knowledge is the impacts of the pandemic on spending power and livelihoods. These data are key not just for design of social safety net transfers but for capturing the demand side impact of COVID-19 on FSCs. I have yet to see any data on this in Africa, other than broad national estimates with some sectoral breakdown based on CGE modeling (e.g. as produced by IFPRI). While useful, these in no way replace real-time information on magnitudes of livelihood loss. Again, cellphone surveys can be a rapid and effective way of generating this data in an ongoing way. To be most useful, they should be done in close collaboration with telecom service provides to generate stratified samples (e.g. between rural and urban areas, and ideally distinguishing between types of cities) and conduct these surveys in very regular fashion
Better modeling fed by better data that drives decision making. This can be done, there is time to do it and to continuously improve the models in real time, and there is definitely need: if done in timely fashion with the right partners, they can have a major impact on the course of this pandemic.