


 Print
Print Email
EmailSince the declaration of COVID-19 as a global pandemic, governments around the world have introduced several measures to restrict social and economic behavior of people to flatten the epidemic peak and lessen the impact on healthcare services. Governments in African countries, in particular, have acted faster and more strictly than other regions at similar early stages of the pandemic. These government efforts to minimize the spread of disease emphasize behavioral interventions, including raising awareness of the disease, and encouraging protective behaviors such as social distancing and hand washing. The success of these government decisions and protective measures rely largely on rapid changes in population behavior, which are dependent on individuals’ ability to perceive risks associated with the virus and adapt their behavior accordingly1. On a continent where a large percentage of workforce is self- employed in the informal sector and 85% of people live on less than $5.50/day, are these measures really effective? Many news stories have reported the brutality associated with the fierce enforcement of coronavirus lockdowns in Africa. Several opinion pieces have raised concerns about whether such measures make sense and experts have questioned the efficacy of these measures. A question underlying these concerns is—will people comply with lockdowns when an individual’s risk of losing his/her livelihood far exceeds the risk of dying from coronavirus?
As a researcher, I was interested in data and evidence to address this question, and to understand the extent to which these drastic measures in Africa are: a) raising awareness about the risk of this disease among people both in urban and rural areas, and b) changing their behavior at the early stages when preventative measures are so crucial. Given the different socio-cultural and economic roles of men and women, I was also interested in understanding differential behavioral responses by gender. I recently came across a dataset, which was not designed specifically for this purpose, but which sheds some light on the awareness of coronavirus, its perceived risk and behavioral responses by people at the early stages of shutdowns in Africa. These data suggest that protective behaviors have changed, but the response varies across countries, and in some countries, it differs by location and gender. I present the data, main results, and discuss limitations and implications from this emerging evidence.
1. Data
The data is from a cellphone-based population survey conducted by Geopoll from April 2nd to April 9th, 2020. The survey was conducted through SMS and mobile web. Thus, data are representative of literate adults with access to a mobile phone. In my blog of April 4, 2020, I discussed the pros and cons of these and other modes of doing surveys using mobile phones in the time of COVID-19 lockdowns and beyond. This dataset is an example of rapid surveys conducted using mobile phones to get a snapshot of the on- the-ground situation and behavioral responses as things were unfolding.
The survey covered 12 countries - Benin, Democratic Republic of Congo (DRC), Ghana, Ivory Coast, Kenya, Mozambique, Nigeria, Rwanda, South Africa, Tanzania, Uganda, and Zambia - that together represent about 57% of the population in Sub-Saharan Africa. The national mobile phone penetration in these 12 countries range from around 50% in Mozambique to 91% in South Africa.2 Data from a total sample of 4,788 individuals was collected with a sample size of 400 in each country except DRC, which had a sample size of 388. More details on the survey methodology, sample description, study report, and an interactive dashboard based on this survey data are available on this webpage.
On March 22, Rwanda had become the first country in sub-Saharan Africa to order a total shutdown. By early April, when this survey was conducted, most of the countries included in this study had put in place localized (e.g., Nigeria, Tanzania, DR Congo, Benin, Ivory Coast, Zambia, Ghana) or national lockdowns (e.g., South Africa, Kenya, and Uganda).3 In this blog, I focus on five questions included in this survey that relate to awareness, risk perception, and safety behavior during the early stages of government actions, and present comparative results by gender and location (urban vs. rural) of the respondent.4
2. Results Awareness
Question 1. Are you aware of the recent global Coronavirus outbreak?
Data suggest that at least in the 12 countries included in the study, there was high level of awareness of coronavirus at the early stages of shutdowns and government interventions (i.e., the week of April 2-9). One hundred percent of respondents across all countries had heard of the global Coronavirus outbreak. This is encouraging, since awareness of a problem is necessary to change individuals’ behavior, which is a crucial step in country’s preparedness for highly contagious pandemics like COVID-19. However, note that all the sampled individuals for this survey had access to a mobile phone, which can be a source of news and information. The level of awareness is likely to be less than 100% among people with no access to mobile phones (i.e., people outside the sampling frame of this survey), which on average across these 12 countries (not weighted by population) is potentially about 23% of population.
Concern/risk perception
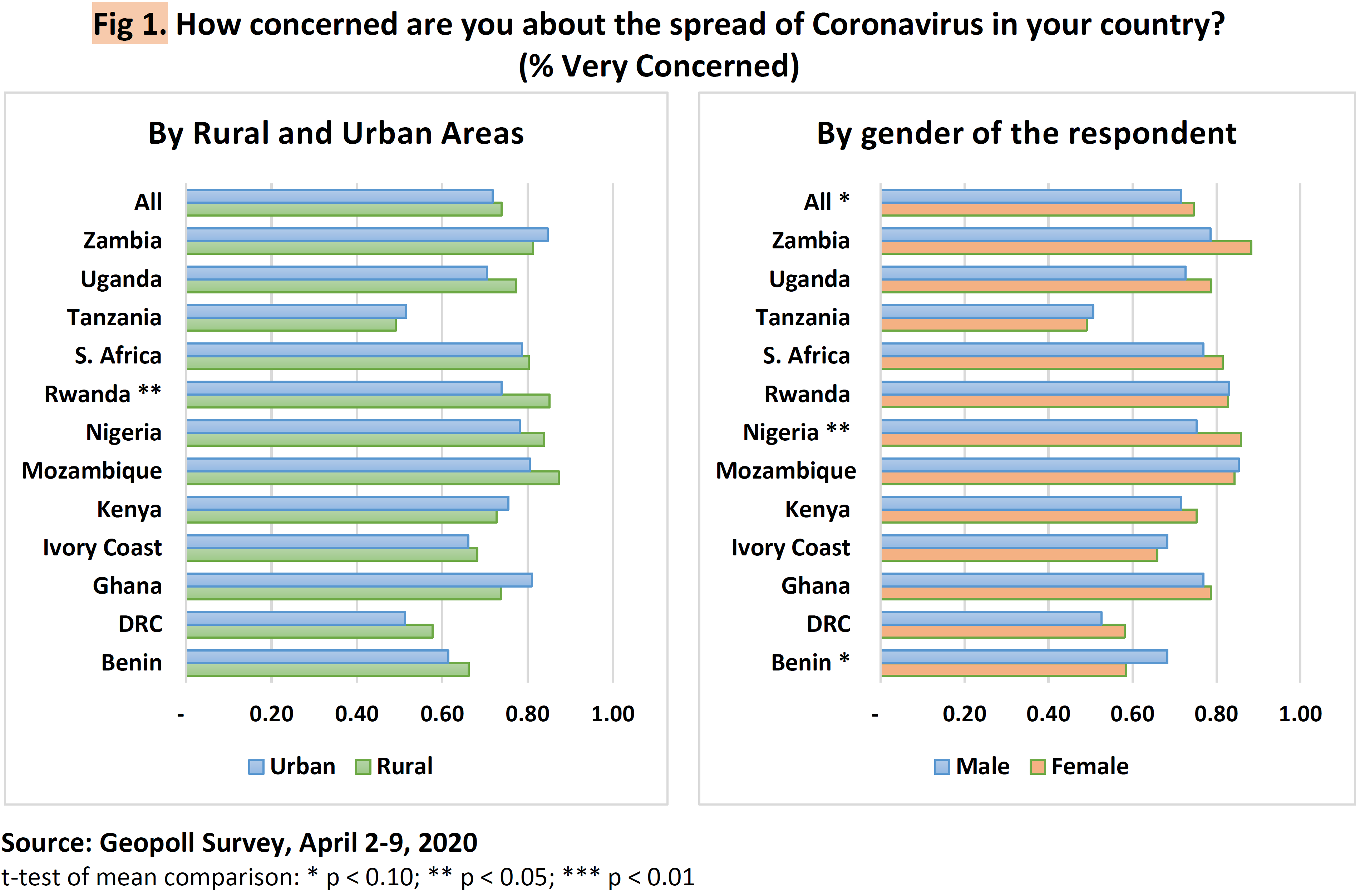
Question 2. How concerned are you about the spread of coronavirus in your country?
Across all 12 countries, 72% of sampled individuals reported a high level of concern about the spread of disease (Fig 1). But there is wide variation across countries. The level of concern was lowest in Tanzania (50%) and highest in Mozambique (82%). In general, the level of concern is not significantly different by respondents’ location. The only exception is Rwanda, where a significantly higher percentage of respondents in rural areas (85%) expressed high level of concerns compared to respondents in urban areas (74%). On average, across all countries, the level of concern was slightly higher among women than men, with this difference statistically significant in Nigeria. However, the opposite was the case in Benin, where significantly more men expressed concerns about the spread of coronavirus in the country than women.
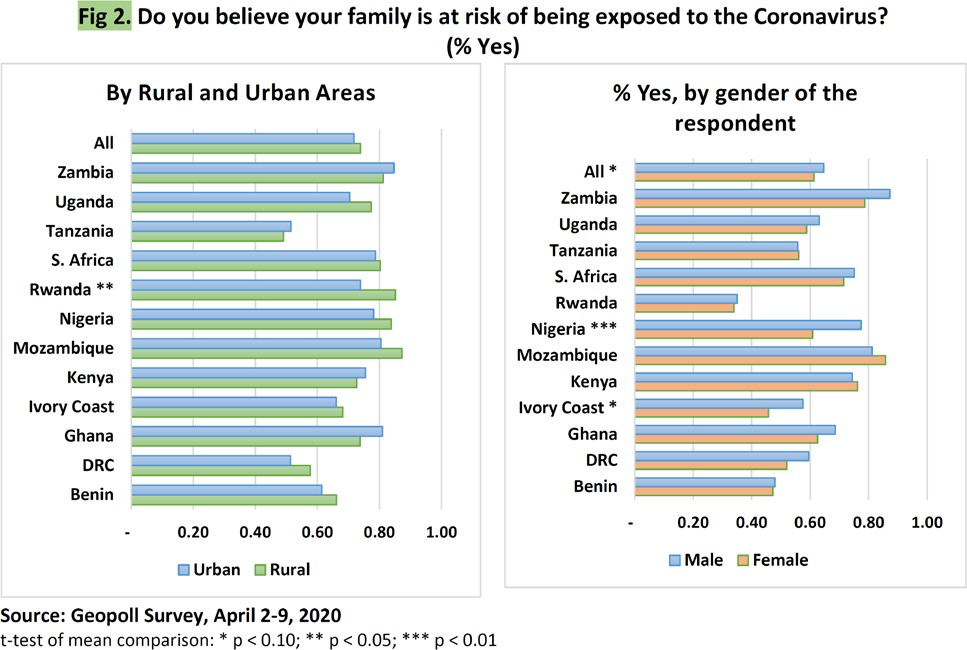
Question 3. Do you believe you or your family are at risk of being exposed to the Coronavirus?
Research suggests that individuals typically tend to underestimate their likelihood of experiencing adverse life events (such as cancer) relative to the average person, an effect known as optimism bias.5 The survey data from these 12 countries demonstrate this effect. The percent of respondents who were very concerned and believed that their family was at risk of being exposed to the coronavirus was on average 10 percentage points lower (63%) than being very concerned about the spread of disease in the country (73%). Again, there is a huge variation in the risk perception by country, with Rwanda at the lower end (where 35% of respondents believe that their family is at risk of being exposed to coronavirus) and Zambia and Mozambique on the higher end (84%).
On average, more men than women were concerned about the risk of family exposure to coronavirus (Fig 2). This difference was statistically significant in West African countries of Nigeria and Ivory Coast.Also, this risk perception of family exposure was greater among urban respondents than it was in rural areas in Uganda and Rwanda. But in all other countries, there was no statistically significant difference in the risk perception of family exposure to coronavirus among rural and urban residents or among men and women.
Safety behavior
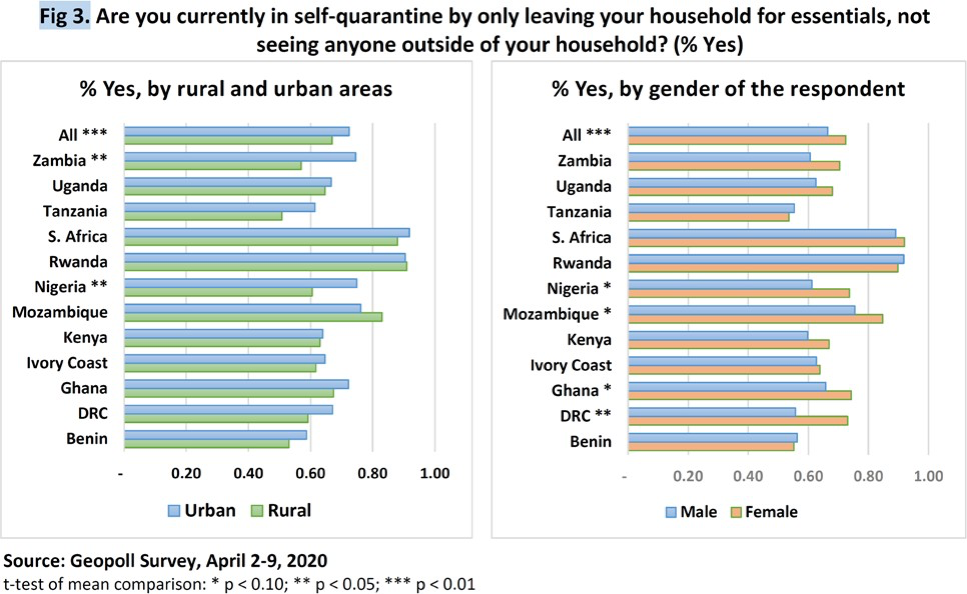
Question 4. Are you currently in self-quarantine?
The main reason for governments taking blunt measures of imposing curfews and lockdowns is to allow people ‘space’ to practice social distancing, which is critical in the case of COVID-19 due to its high transmissibility, even in the absence of symptoms. In the week of April 2-9, 70% of people across the 12 countries surveyed indicated that they were practicing self-quarantine and leaving the house only for essentials (Fig 3). This practice of social distancing varied from 54% in Tanzania (which had only imposed localized lockdowns) at the lower end to 91% in Rwanda and South Africa, which were among the first few countries to impose national lockdowns in SSA. On average, across all countries, significantly more respondents in urban areas were practicing self-quarantine than in rural areas, and this difference was more pronounced in Zambia and Nigeria. Also, on average more women than men reported practicing self-quarantine and leaving the house only for essentials. The difference in the practice of social distancing between men and women was significant in Nigeria, Mozambique, Ghana and DRC. The different levels of self-quarantine observed in rural and urban areas and among men and women could reflect cultural norms and economic roles. But it could also be due to measures taken or not taken by the governments. For example, countries where the differences between men and women, and between rural and urban areas was statistically significant are all countries where the governments had not imposed any national lockdowns as of the end of March.6
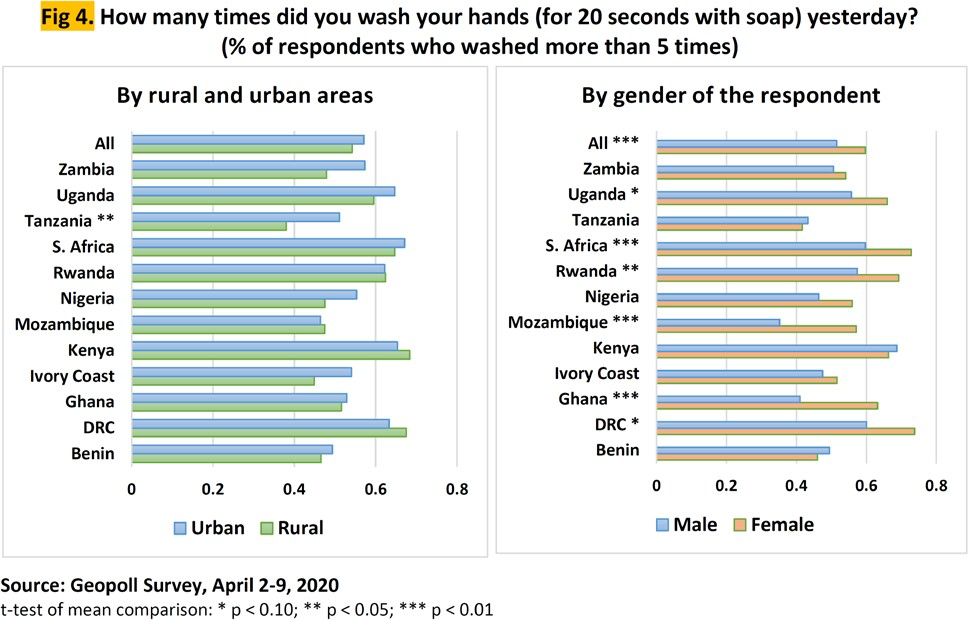
Question 5. How many times did you wash your hands (for 20 seconds with soap) yesterday?
Hands are an easy pathway for the bacteria and viruses to enter the body through eyes, nose, and mouth. Thus, more frequent hand washing with soap for at least 20 seconds is the universal message promoted by the national and international public health agencies and organizations. Thus, the survey included a question on the number of times a person washed their hands for 20 seconds with soap the previous day, with options of zero times, 1-2 times, 3-5 times, and more than 5 times. The recommendation is to wash hands often. The exact number of times a person should wash their hands depends on the activities he/she does and the number of times a person uses the toilet throughout the day. It is well recognized that measurement of hand washing by self-report risks substantial overestimation of the behavior both in terms of number of times per day and number of seconds per hand wash.7 Despite this risk of overestimation, I report the results for responses of ‘more than 5 times,’ as six times seems to be the least number of times a person should be washing hands in 24 hours even in a normal day.
Data suggest that about 55% of respondents across the 12 countries reported washing hands with soap more than 5 times with a wide range across countries (Fig 4). Thirty eight percent of respondents from rural Tanzania reported washing hands more than 5 times, which was the lowest across all countries, and significantly lower than respondents from urban Tanzania. Research suggests that less wealthy households and households in rural areas are less likely to have soap and water than wealthy households and those in urban areas.8 In fact, data from the most recent Demographic and Health Surveys (DHS) (from 2011 to 2018) indicate that only 22% of population across these 12 countries lived in households with a basic hand washing facility with soap and water. For households in the lowest and the highest wealth quintiles, the average was 9% and 46%, respectively.9
The lack of access to a basic hand washing facility in many rural and poor households as shown by the DHS data, thus raises the question--are the self-reported hand washing numbers credible, or are people reporting what they believe they are supposed to be doing? My quick and un-exhaustive search for prior research did not yield much in terms of data or evidence on the frequency of hand washing in the African or other developing country context.10 But I did find a couple of surveys in developed countries where respondents had self-reported the frequency of hand washing, which provides a good benchmark. For example, data from a survey conducted by the Behavioural Insights Team of 2,600 UK adults last month (between March 12-17) suggest that 59% of respondents self-reported washing hands 6 or more times with soap and water or a hand sanitizer the previous day. In a survey conducted in the U.S. in 2009 by the American Cleaning Institute, about 88% of adults had reported washing hands five or more times a day, and 53% had reported spending more than 15 seconds lathering the soap or rubbing the hands with soap. These estimates of self-reported frequency of handwashing in high income countries where handwashing facility is less likely to be a limiting factor, are less than the averages reported for many African countries in the Geopoll survey (Fig 4). This makes me believe that the self-reported handwashing behavior in this Geopoll survey could be significantly biased upwards.
If the upward bias is equally affecting self-reports by men and women, one thing the Geopoll data confirms is the gender difference in this important safety measure. Men reported this practice significantly less than women across several countries (i.e., DRC, Ghana, Mozambique, Rwanda, and Uganda), including a relatively wealthy country like South Africa. Only 35% of men in Mozambique reported washing hands more than 5 times the previous day, which is the lowest across all countries surveyed. It is also significantly lower than 57% reported by women counterparts in Mozambique. Gender seems to be an important factor for handwashing in general across all countries and cultures.11 In the March 2020 UK survey mentioned above, 50% of men reported washing hands six or more times the previous day compared to 67% of women.
3. Insights and implications from this data and analysis
The Geopoll survey data indicate that cellphone owners in rural areas of Africa are as informed as urban areas; and women are as informed as men about the global coronavirus pandemic. With a few exceptions, the level of concern about the spread of this disease was equally shared by people residing in rural and urban areas, and by men and women. This demonstrates the success of government efforts in raising general awareness of the disease and the level of concerns about the spread of the disease across the population in the early stages of shutdowns. However, there is a wide variation across countries in the risk perception of family exposure to coronavirus with no clear correlation with government measures taken or not taken by early April. For example, the perceived risk for family exposure to this disease was the lowest in Rwanda which was one of the first countries to impose national lockdown, but it was much higher in South Africa, Kenya and Uganda, which had also imposed national lockdowns within days of its imposition in Rwanda. This shows that other factors such as the actual confirmed cases, number of deaths due to coronavirus, trust in the government or healthcare system may be influencing risk perceptions of someone from the family getting infected by the disease. It is also possible that these differences across countries could be a reaction to the government force imposed to enforce the lockdowns and the direct or implicit fear of government retributions by respondents in some countries.
The data also shows wide variation among countries in protective behaviors such as social distancing and hand washing. Social distancing was highest in countries that were early adopters of national lockdowns. It was relatively higher in urban vs. rural areas and among women than men. Similar pattern is observed for hand washing behavior. The most striking result is the gender difference in hand washing behavior, with men practicing this protective measure significantly less than women across several countries, including a relatively wealthy country like South Africa.
Adaptation of behavior will be fundamental to the management of this pandemic in Africa and elsewhere. This quick analysis of a publicly available dataset demonstrates the need to promote safety measures and outreach efforts to target groups like people living in rural areas and to men who are less likely to engage in protective measures like social distancing and hand washing compared to women. It also points to the need for more timely research to characterize psychological and behavioral responses across the globe during pandemics in order to recommend and implement the most optimal strategies for effecting behavioral change, which often are culturally specific.
Footnotes
1Xu J, Peng Z. People at Risk of Influenza Pandemics: The Evolution of Perception and Behavior. PLoS ONE. 2015;10(12):e0144868.
2For the other 10 countries in this study, these estimates are: Benin (82%), DRC (80%), Ivory Coast (80%), Kenya (80%), Nigeria (80%), Rwanda (76%), Tanzania (75%), Uganda (71%), and Zambia (82%). These estimates are based on the study by the Pew Research Center and data reported on Statistica website. A simple arithmetic mean of mobile penetration across all 12 countries in this study is 77%.
3Source (accessed on April 24, 2020): https://www.bbc.com/news/amp/world-52103747
4Data are weighted by population-based statistics on gender, age group, socio-economic class, and rural/urban split to make them closely representative of population characteristics at the country level.
5Sharot T. The optimism bias. Current Biology. 2011 Dec 6;21(23):R941–5.
6Source (accessed on April 24, 2020): https://www.bbc.com/news/amp/world-52103747
7See for example, Biran A, Rabie T, Schmidt W, Juvekar S, Hirve S, Curtis V, 2008. Comparing the performance of indicators of hand-washing practices in rural Indian households. Trop Med Int Health13: 278–285
8Kumar, S.; Loughnan, L.; Luyendijk, R.; Hernandez, O.; Weinger, M.; Arnold, F.; Ram, P.K. Handwashing in 51 countries: Analysis of proxy measures of handwashing behavior in multiple indicator cluster surveys and demographic and health surveys, 2010–2013. Am. J. Trop. Med. Hyg. 2017, 97, 447–459.
9Data accessed on April 29, 2020 from: https://www.statcompiler.com/en/.
10This is not to imply that there is limited research on the topic of handwashing. In fact, the following publication by the Global Handwashing Partnership summarizes 117 handwashing related research papers published in 2017: https://globalhandwashing.org/resources/2017-handwashing-research-summary/.
11See this blog by Rebecca Onion on “The long history of the handwashing gender gap” for a nice historical overview of why women are slightly better in handwashing then men.
